VA said to keep lid on whistle-blowers
Tuesday, June 24, 2014
WASHINGTON -- A top federal investigator has identified "a troubling pattern of deficient patient care" at Veterans Affairs facilities around the country that she says was pointed out by whistle-blowers but downplayed by the department.
The problems went far beyond the long wait time for some appointments -- and the attempts to cover them up -- that has put the department under scrutiny.
In a letter Monday to President Barack Obama, Carolyn Lerner of the U.S. Office of Special Counsel cited canceled appointments with no follow-up, drinking water contaminated with the bacteria that causes Legionnaires' disease, and improper handling of surgical equipment and supplies.
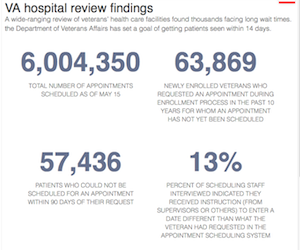
Acting VA Secretary Sloan Gibson said he had launched a departmental review due to be completed within 14 days. "I am deeply disappointed not only in the substantiation of allegations raised by whistle-blowers, but also in the failures within VA to take whistle-blower complaints seriously," he said in a statement.
Lerner said the VA consistently acknowledges problems but says the quality of patient care is not affected, which she referred to as "the VA's typical harmless error approach."
"This approach has prevented the VA from acknowledging the severity of systemic problems and from taking the necessary steps to provide quality care to veterans," Lerner wrote to Obama. "As a result, veterans' health and safety has been unnecessarily put at risk."
Complaints about a lack of access to VA health care have prompted a national outcry that led to VA Secretary Eric Shinseki's resignation. The most startling allegations have arisen out of the VA's medical center in Phoenix, where a VA inspector general's investigation found that about 1,700 veterans in need of care were "at risk of being lost or forgotten" after being kept off an official electronic waiting list.
Lerner says the office is reviewing more than 50 complaints alleging threats to patient health and safety and has referred 29 of them to the VA for investigation.
Her office is an independent investigative and prosecutorial agency that protects federal workers from prohibited personnel practices, especially reprisal for whistle-blowing.
Lerner said two cases highlight her concerns. In Fort Collins, Colo., the VA's Office of Medical Inspector confirmed multiple violations of policy concerning appointment scheduling and cancellations that masked true wait times. Nearly 3,000 veterans were unable to reschedule canceled appointments, and one nurse practitioner alone had 975 patients unable to reschedule appointments. However, the same office did not substantiate that the failure to properly train staff resulted in danger to public health and safety.
Lerner said the VA's conclusion "is not only unsupportable on its own, but is also inconsistent with reports by other VA components examining similar patient-care issues."
In a second case, a VA psychiatrist disclosed concerns about patient neglect in a long-term mental health care facility in Brockton, Mass. One veteran who was a resident of the facility between 2005 and 2013 had only one psychiatric note written in his chart. Another was admitted to the facility in 2003, yet his first comprehensive psychiatric evaluation did not occur until 2011.
Despite the findings, the VA said there was no effect on patient care. A follow-up was requested, and the VA again said it did not feel that the patient's rights were violated.
She cited other cases in Buffalo, N.Y.; Little Rock; Harlingen, Texas; Jackson, Miss., and San Juan, Puerto Rico, to bolster her position that the VA is downplaying the effect of deficient care.
Both the House and Senate have passed legislation that would require the VA to pay private providers to treat qualifying veterans who can't get prompt appointments. Each chamber has appointed a committee to iron out differences between the two bills, with the lawmakers meeting today.
VETERANS
A Section on 06/24/2014