WASHINGTON - Medicaid embarked on a transformation Wednesday from a safety-net program for the most vulnerable to a broad based one that finds itself at the front lines of the continuing political and ideological battle over the Patient Protection and Affordable Care Act.
Already the nation’s largest health-care program, Medicaid is being expanded and reshaped by the law to cover more people.
Among them will be many who consider themselves middle class - people like Sandy Kush, who initially bristled when she learned that she would be joining a program she had always thought of as being only for the poor.
“Maybe it’s like a shame thing. I was raised middle class. I own my house. It just seems like not me,” said Kush, 49, an unemployed medical transcriptionist in Naperville, Ill., who said she would have preferred to buy a private health plan with the help of a federal subsidy.
On Wednesday, people who signed up for coverage under the new law will be able to use it, in what supporters have hailed as a historic moment for health care in the United States.
So far, more than 2 million Americans, many previously uninsured, have enrolled in private health plans, thanks in large part to new federal subsidies for low- and middle-income people to buy coverage.
The program’s Oct. 1 launch was deeply flawed, and people’s difficulties in navigating the system have dominated headlines.
Far more people - about 3.9 million - took steps in October and November to sign up for Medicaid, according to federal figures. That includes people who became eligible for the state-federal program under the expansion, as well as those who could have enrolled previously, but for one reason or another did not signup until now.
Twenty-five states - including Arkansas - and the District of Columbia expanded Medicaid under the Affordable Care Act. In many of those places, the program will be open for the first time to anyone whose income is below 138 percent of the poverty level - individuals making less than $15,856 a year or a family of four earning under $32,499 in 2013 dollars. That includes childless adults, who were excluded in most states despite a widely held misperception that all poor people automatically qualified for Medicaid.
“The big change is that it really is going to operate the way most people thought it did,” said Judy Solomon, a Medicaid expert at the Center on Budget and Policy Priorities, a think tank focused on policies affecting low- and moderate-income people.
The newly eligible in the expanded-Medicaid states come from many strata of society: homeless people, former inmates, low-paid workers, recent college graduates, retirees not yet old enough for Medicare and people like Kush, who are between jobs.
In the states that rejected the expansion, Medicaid will largely remain limited to groups of people who traditionally have been covered by the program: children, pregnant women, very-low-income parents, and the poor elderly and disabled.
Even in states that aren’t expanding Medicaid, there are some significant changes, including new Medicaid eligibility standards. For people who are not in long-term care, the program will no longer take into consideration how much participants have in assets, such as savings or retirement accounts.
Medicaid already covers about 16 percent of the U.S. population - more people than Medicare, the federal health program for people 65 and over. That includes 31 million children, nearly 9 million disabled adults under age 65 and more than 4.6 million low-income senior citizens.
It finances 40 percent of all the births in the United States and is the largest source of coverage for Americans who have HIV and AIDS. More than 60 percent of those living in nursing homes are covered by Medicaid.
Supporters of the healthcare law say that expanding Medicaid is a critical part of the effort to reduce the ranks of the uninsured and will build acceptance for a program that has been stigmatized since its inception in 1965 as essentially a fringe benefit for those on public assistance.
“Medicaid - for all the good we think it does, and it does do a lot of good - it does have a connotation,” said Matt Salo, executive director of the National Association of Medicaid Directors.
Rep. Henry Waxman, D-Calif., one of Medicaid’s leading champions in Congress, said that as a result of the expansion, “we’ll see a whole lot of grateful Americans, and a whole lot more support for Medicaid, in areas where it has traditionally been scorned as a poor people’s program.”
But critics say the growth of the program will merely foster government dependency.
“I think it is very bad social welfare policy,” said Edmund Haislmaier, a senior research fellow at the Heritage Foundation. “You are taking people who are by and large young, healthy and perfectly capable productive members of society and encouraging them to become dependent on public assistance. This is the very last population you want to do that for.”
Medicaid was created as part of the same law that established Medicare. States were given the option to participate. Within seven years, all had joined except Arizona, which did not climb aboard until 1982. Although states were required to cover certain groups such as low-income children, they traditionally have had broad leeway in running their programs.
Because of its roots as a welfare program, Medicaid has long had an image problem. In the past, states that have expanded the program have felt compelled to rebrand it - as BadgerCare in Wisconsin, for example, and SoonerCare in Oklahoma.
President Barack Obama and many Democratic lawmakers initially resisted the Medicaid expansion that became part of the Affordable Care Act. But it turned out to be significantly less expensive than providing federal subsidies to lower-income people to buy private health insurance through the state and federal exchanges.
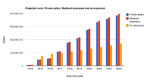
The law, as enacted in 2010, required all 50 states to expand Medicaid to reach the goal of extending coverage to 30 million uninsured Americans over the next decade. But the Supreme Court ruled in June 2012 that states could not be compelled to expand their programs. Because so many states rejected the expansion, the Congressional Budget Office estimated in 2012 that 6 million fewer would enroll in Medicaid over the next decade than initially expected.
States that are led by Democrats have rushed to embrace the Medicaid expansion, as have a small number of states governed by Republicans.
The decision by many states to reject the Medicaid expansion has thwarted a basic goal of the law, which is to make health-care coverage universal and affordable. In the nonexpansion states, people just above the poverty line are eligible for subsidies for private insurance, while those below it are not, and thus get no benefit from the Affordable Care Act.
States opposed to the Medicaid expansion say that billions in new federal funds, which will cover almost all the cost of the newly eligible for several years, will eventually dry up, saddling states with enormous costs and the politically dicey prospect of having to toss people off the Medicaid rolls.
Beyond fiscal concerns are philosophical ones. When Senate Minority Leader Mitch McConnell, R-Ky., was asked recently about the brisk rate of health-coverage enrollment in his state, he said most people were simply jumping at a government handout.
“Well, 85 percent of the people who’ve signed up in Kentucky have signed up for Medicaid,” he said. “That’s free health care. If you want to give out free health care, you’re going to have a lot of interest. Just like free anything else.”
One of McConnell’s constituents, Sharon Kelly of Louisville, sees it differently. She was so eager to get coverage that she got online at 12:15 a.m. on Oct. 1, just 15 minutes after program enrollment opened. A former home-health aide who made $12 an hour working with elderly people, she has been without insurance since she lost her last long-term job in 2009. She previously wasn’t eligible for Medicaid in Kentucky because she does not have a dependent child.
Kelly said that having Medicaid coverage on Jan. 1 “is a huge relief,” adding, “I’m a redhead and I used to live in California. I have things on my skin that are probably cancer. I just sit here watching these things change color, waiting for January 1st, so I can get an appointment with a dermatologist.”
Even supporters of the law, however, concede that adding so many additional people to Medicaid raises worrisome possibilities.
Already, some Medicaid recipients complain that they cannot find doctors and other health-care providers who are willing to accept the program’s low reimbursement rates.
While the law temporarily boosts what primary-care providers receive for seeing Medicaid patients - to the same rates they get from Medicare - the increase lasts only until the end of 2014.
Waxman and others also are concerned that it could be difficult for Medicaid recipients to find specialists, whose compensation will not be increased under the law.
Still, there are those who say they prefer Medicaid to private insurance. Among them is Chris Confalone, 25, of Clifton, N.J., a $15,000-a-year library worker who has not had health insurance since he graduated from high school in 2006.
“The one good thing about Medicaid is it’s coming through the government,” he said. “I feel a little more comfortable going through the state rather than a private company.” Information for this article was contributed by Alice Crites of The Washington Post.
Front Section, Pages 1 on 01/02/2014